
ABSTRACT
Introduction and objectives: Ultrasound renal denervation (uRDN) has emerged as an innovative therapeutic approach for the treatment of hypertension. However, its efficacy compared to medication remains uncertain. We aimed to assess the efficacy profile of uRDN vs sham groups focusing on its impact on daytime ambulatory blood pressure, 24-hour blood pressure, home blood pressure and office blood pressure.
Methods: We conducted a systematic search across Embase, PubMed, and Cochrane Library databases from their inception up 1 November 2024 to identify randomized controlled trials evaluating the efficacy of uRDN. Statistical analyses were performed using RevMan 6.3 software, utilizing the mean and standard deviation method to calculate mean differences with a 95% confidence interval (95%CI).
Results: A total of 4 studies were included in the final analysis with 642 patients. uRDN significantly reduced daytime ambulatory systolic blood pressure (SBP) (−5.12 mmHg; 95%CI, −6.07 to −4.16; P ≤ .00001), 24-h SBP (−4.87 mmHg; 95%CI, −6.53 to −3.21]; P ≤ .00001), office SBP (−5.03 mmHg; 95%CI, −6.27 to −3.79; P ≤ .00001) and showed a decrease in patient medication 6 months after the procedure.
Conclusions: Using uRDN leads to a lower blood pressure in patients within 2 months following the procedure. Additionally, after 6 months a significant decrease in drug use is observed.
This meta-analysis protocol was registered on PROSPERO on 7 July 2024 (CRD42024562852).
Keywords: Resistant hypertension. Ultrasound renal denervation. Systolic blood pressure. Diastolic blood pressure. Antihypertensive treatments.
RESUMEN
Introducción y objetivos: La denervación renal por ultrasonido (DRU) ha surgido como un enfoque terapéutico innovador para la hipertensión arterial resistente. Sin embargo, su eficacia en comparación con la medicación sigue siendo incierta. Nuestro objetivo fue evaluar la eficacia de la DRU frente a grupos simulados, con especial atención a su impacto sobre la presión arterial ambulatoria diurna, la presión arterial de 24 h, la presión arterial domiciliaria y la presión arterial en el consultorio.
Métodos: Se realizó una búsqueda sistemática en las bases de datos Embase, PubMed y Cochrane Library hasta el 1 de noviembre de 2024, para identificar ensayos controlados aleatorizados que evaluaran la efectividad de la DRU. Los análisis estadísticos se realizaron con el programa informático RevMan 6.3, utilizando la media y la desviación estándar para calcular las diferencias de medias con un intervalo de confianza del 95% (IC95%).
Resultados: En el análisis final se incluyeron cuatro estudios con 642 pacientes. La DRU redujo de manera significativa la presión arterial sistólica (PAS) ambulatoria diurna (−5,12 mmHg; IC95%, −6,07 a −4,16; p ≤ 0,00001), la PAS de 24 h (−4,87 mmHg; IC95%, −6,53 a −3,21; p ≤ 0,00001) y la PAS en la consulta (−5,03 mmHg; IC95%, −6,27 a −3,79; p ≤ 0,00001), y logró una disminución de la medicación de los pacientes a los 6 meses del procedimiento.
Conclusiones: El uso de DRU conlleva una reducción de la presión arterial a los 2 meses del procedimiento. Adicionalmente, transcurridos 6 meses se observó una disminución significativa del uso de medicación.
El protocolo de este metanálisis fue registrado en PROSPERO el 7 de julio de 2024 (CRD42024562852).
Palabras clave: Hipertensión resistente. Denervación renal por ultrasonido. Presión arterial sistólica. Presión arterial diastólica. Tratamiento antihipertensivo.
Abbreviations
BP: blood pressure. DBP: diastolic blood pressure. SBP: systolic blood pressure. RCT: randomized controlled trial. uRDN: ultrasound renal denervation.
INTRODUCTION
Hypertension is highly prevalent worldwide and well recognized as a major risk factor for cardiovascular, cerebrovascular, and renal complications.1 Despite the availability of numerous antihypertensive drugs that effectively mitigate hypertension-related organ damage,1,2 a substantial proportion of patients fail to attain adequate blood pressure (BP) control,3 which may be attributed to factors such as medication non-adherence or the presence of resistant hypertension,4,5 which is defined as the presence of uncontrolled BP of, at least, 130/80 mmHg despite the simultaneous prescription of, at least, 3 or 4 antihypertensive drugs of different classes, or controlled BP despite the prescription of, at least, 4 drugs, at the maximum tolerated doses, including a diuretic.6 The pathophysiology of hypertension is intricate and includes a diverse array of mechanisms, with sympathetic overdrive emerging as a pertinent factor in all forms of hypertension.7 Consequently, novel therapeutic approaches have emerged, including renal denervation (RDN), which aims to decrease renal sympathetic activity thereby reducing BP. RDN has drawn considerable attention as a guideline-recommended BP lowering treatment along with lifestyle changes and pharmacotherapy for patients with resistant hypertension.8,9 Recently, there has been growing consensus that RDN should also be considered for individuals whose hypertension is due to no therapeutic adherence.10-12 Early randomized controlled clinical trials yielded inconsistent findings on the efficacy profile of the intervention, with a substantial proportion of patients failing to respond across the trials.13,14 Potential explanations for the heterogeneous results include insufficient operator experience using the Symplicity Flex catheter (Medtronic, United States), the study participants’ baseline characteristics, and changes of antihypertensive medication.15 Subsequently, sham-controlled trials with better study designs, catheter technologies and procedural techniques have improved the BP-lowering safety and efficacy profile of RDN.16-18 Currently, various catheter systems are used for RDN, utilizing different technologies, such as radiofrequency-based systems like Symplicity Spyral (Medtronic, United States). Ultrasound-based catheters have also been developed, such as the Paradise (Recor Medical, United States), whose efficacy has been evaluated in multiple studies. Finally, there is a system based on alcohol-mediated RDN.19 Recently, the U.S. Food and Drug Administration (FDA) approved Medtronic Symplicity Spyral and Recor Paradise system as adjuvant therapies for the treatment of hypertension.20
The efficacy of the latter was evaluated in a multicenter, randomized, blinded and sham-controlled trial. Subsequently, it was determined in the REQUIRE RADIANCE-HTN SOLO,16 RADIANCE HTN TRIO17 and RADIANCE II,18 and REQUIRE21 trials. Results were heterogeneous between the RADIANCE and REQUIRE trials, which had limitations that may account for the varied results.10 Finally, uRDN was concluded to be safe for the treatment of hypertension, even in patients with resistant hypertension and poor medical adherence.19 The aim of this study is to conduct a systematic review and a meta-analysis to examine the antihypertensive efficacy of uRDN in patients with hypertension vs a sham group treatment.
METHODS
We conducted a systematic review and meta-analysis which strictly followed the clinical practice guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.22 Methodological procedures were conducted in full compliance with the Cochrane Handbook of Systematic Reviews and Meta-Analysis of Interventions. This meta-analysis protocol was registered on PROSPERO 7 July 2024, under protocol ID: CRD42024562852.
Criteria of the included studies
Inclusion criteria were established to identify relevant studies: patients with resistant hypertension and randomized controlled trials (RCTs) comparing uRDN with sham groups, which did not undergo uRDN; RCTs reporting office, daytime ambulatory, home and 24-h ambulatory BP changes from baseline were included. We excluded those underreporting, at least, 1 of the following outcomes of interest: changes in BP between baseline and, at least, a 2-month follow up. In addition, we excluded non-English publications, case-control studies, case reports, single arm studies, letters to the editors, basic science research, meta-analyses, and review articles.
Literature search strategy
We conducted a comprehensive search across PubMed, EMBASE, and COCHRANE, from their inception until 1 November 2024. Keywords and free-text terms were used to explore literature on hypertension, renal denervation, and ultrasound ablation. Detailed search information for each database is provided in the Search strategy section of the supplementary data.
Screening of literature search strategy
Initially, a comprehensive database search was conducted to compile all relevant records. Duplicate entries were, then, manually removed using Zotero software. Afterwards, references were screened by title and abstract. When necessary, a full-text review was performed to ensure relevance and accuracy. Two authors (C. J. Palomino-Ojeda and L. H. García-Mena) independently assessed each the inclusion and quality of each article. Discrepancies were resolved by a third author (J. M. Guerrero-Hernández). Additionally, references cited in the included studies were scrutinized and included if they fulfilled the eligibility criteria.
Data extraction
Data extraction was conducted using Excel spreadsheets to record the following information: a) baseline characteristics of the study population, b) summaries detailing the characteristics of the included studies, c) outcome measures, and d) domains evaluated for quality assessment.
Assessing the risk of bias
Randomized controlled trials were assessed using Version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2)22,23 from the Cochrane Handbook of Systematic Reviews of Interventions. Our analysis included a funnel plot for the primary endpoint daytime ambulatory systolic blood pressure (SBP) shown in figure 1 of the supplementary data.

Figure 1. PRISMA flow diagram. RDN, renal denervation.
Outcome measures
BP changes were assessed by comparing baseline values and follow-up measurements taken, at least, 2 months later. The mean difference was analyzed using the mean and standard deviation.
Data analysis
The efficacy profile of uRDN vs the sham control was analyzed using continuous data to calculate the mean difference with its corresponding 95% confidence interval (95%CI).24 This analysis assessed BP changes across groups with an, at least, 2-month follow-up while evaluating their mean difference.
Furthermore, an examination was conducted to discern any variation among office BP, ambulatory daytime BP, 24-h ambulatory BP, nighttime ambulatory BP, and home BP outcomes in trials that reported these results. This was achieved by computing the mean and its associated standard deviation for the difference between the 2 outcomes. The validated Campbell calculator was used to convert the measures of dispersion from the outcomes in the REQUIRE trial for data analysis.24 The level of heterogeneity was assessed using the I2 statistic.
Sensitivity analyses were conducted using a random effects model to account for variability among studies.25 Subgroup analyses were predefined for first and second-generation RDN trials, with tests for interaction for the primary endpoint.
Assessment of heterogeneity
Heterogeneity among the included studies was assessed using Cochran’s Q statistic. Additionally, the I2 statistic was used to quantify the proportion of total variation attributed to heterogeneity, with values > 50% indicating high heterogeneity. All statistical analyses (including the calculation of standardized mean difference, relative risk, and mean difference) were performed using RevMan 6.3. software.22
RESULTS
Study selection
A total of 448 studies were identified across database searches. A total of 392 studies were screened after removing duplicate studies, 388 of which were excluded due to single-arm study (n = 6); publication in a language different than English (n = 1); case-control or case report studies and literature review (n = 140); basic scientific research (n = 24); editorial letter (n = 8); different type of RDN studies (n = 83); studies with ≤ 10 participants (n = 6); and does not compare intervention of interest (n = 120). Finally, 4 studies meet all inclusion criteria and were eligible for analysis. An analysis of 642 patients from the 4 selected articles was conducted as they met the inclusion criteria. The PRISMA flow diagram of the study selection process is shown in figure 1.
Study characteristics
The studies included in our analysis included a total of 4 RCTs published from 2018 through 2023.16-18,21 All studies used uRDN and a sham control group. Two studies were performed in the United States/Europe,16,17 1 study only in the United States18 and the rest in Japan and South Korea.21 The baseline characteristics of the included studies were analyzed and summarized in table 1. Characteristics of the entire patient population are shown in table 2.
Table 1. Baseline characteristics and following intervention of the included studies population.
| Reference | ||||||||
|---|---|---|---|---|---|---|---|---|
| RADIANCE HTN SOLO 201816 | RADIANCE-HTN TRIO 202117 | REQUIRE 202221 | RADIANCE II 202318 | |||||
| Group | uRDN | SHAM control | uRDN | SHAM control | uRDN | SHAM control | uRDN | SHAM control |
| N | 74 | 72 | 69 | 67 | 69 | 67 | 150 | 74 |
| Gender, female | 28 | 33 | 13 | 14 | 21 | 14 | 47 | 17 |
| Gender, male | 46 | 39 | 56 | 53 | 48 | 53 | 103 | 57 |
| Age, years, mean (SD) | 54.4 (10·2) | 53.8 (10·0) | 52.3 (7.5) | 52,8 (9.1) | 50.7 (11.4) | 55.6 (12.1) | 55.1 (9.9) | 54.9 (7.9) |
| Body mass index, mean (SD) | 29.9 (5.9) | 29.9 (5.0) | 32.8 (5.7) | 32.6 (5.4) | 29.5 (5.5) | 28.4 (4.5) | 30.1 (5.2) | 30.6 (5.2) |
| Abdominal obesity | 41 | 44 | 54 | 55 | – | – | 90 | 46 |
| GFR mL/min/1.73 m2 | 84.7 (16.2) | 83.2 (16.1) | 86 (25.2) | 82.2 (19.2) | 74.2 (16.2) | 69.6 (17.1) | 81.4 (14.4) | 82.3 (14.9) |
| GFR < 60 mL/min/1.73 m2 | 1 | 3 | 8 | 7 | 15 | 18 | 7 | 3 |
| Type 2 diabetes mellitus | 2 | 5 | 21 | 17 | 18 | 20 | 9 | 5 |
| Cardiovascular disease | – | – | 8 | 9 | 9 | 9 | 1 | – |
| Systolic BP at office screening, mm Hg | 142.6 (14.7) | 144.6 (15.9) | 161.9 (15.5) | 163.6 (16.8) | 157.6 (19.5) | 160.4 (14.9) | 155.8 (11.1) | 154.3 (10.6) |
| Diastolic BP at office screening, mm Hg | 92.3 (10.1) | Mean 93.6 (8.3) | 105.1 (11.6) | 103.3 (12.7) | 97.7 (16.6) | 95.3 (14.2) | 101.3 (6.7) | 99.1 (5.6) |
| HR at office screening, beats/min | 72 (12.1) | 72.6 (12.3) | 74.5 (11) | 77.6 (12.9) | 75.3 (10.8) | 71.5 (12.8) | 74.1 (12.0) | 73.6 (11.9) |
| Number of antihypertensive drugs at screening | 1: 33 2: 28 3: 1 | 1: 28 2: 27 3: 1 | 3: 27 4: 22 5: 20 | 3: 28 4: 24 5: 15 | 3: 32 4: 20 5: 17 | 3: 29 4: 23 5: 15 | 1: 52 2: 44 > 2: 0 | 1: 25 2: 25 > 2: 1 |
| Procedural time | 72.3 (23.3) | 38.2 (12.6) | 83.66 (22.71) | 41.33 (12.87) | 86.7 (54.0) | 40.2 (11.6) | 76.7 (25.2) | 43.9 (16.6) |
| Office systolic blood pressure at 2 months | 143.7 (16.7) | 149.7 (17.4) | 147.1 (20.3) | 152.1 (22) | – | – | 145.8 (15.9) | 151.2 (16.4) |
| Office diastolic blood pressure at 2 months | 94.2 (10.1) | 98 (10) | 96.6 (13.9) | 98.7 (13.8) | – | – | 96.0 (10.2) | 98.1 (11.2) |
| Daytime ambulatory systolic BP at 2 months | 141.9 (11.9) | 147.9 (13.3) | 141.0 (16.1) | 146.3 (18.8) | – | – | 135.6 (13) | 142.9 (10.5) |
| Daytime ambulatory diastolic BP at 2 months | 87.9 (7.1) | 90.9 (7.9) | 88.5 (11.6) | 90.7 (12.2) | – | – | 83.1 (7.6) | 87.0 (6.3) |
| 24-hour systolic BP at 2 months | 135.6 (11.4) | 140.7 (11.8) | 135.2 (16.0) | 140.5 (18.7) | – | – | 135.6 (13.0) | 142.9 (10.5) |
| 24-hour diastolic BP at 2 months | 83 (6.8) | 85.7 (7.1) | 83.6 (10.9) | 85.8 (12) | – | – | 83.1 (7.6) | 87.0 (6.3) |
| Home systolic BP at 2 months | 139.4 (11.7) | 146.6 (15.4) | 144.6 (18.2) | 149.9 (18.9) | – | – | 143.4 (12.3) | 148.8 (12.3) |
| Home diastolic BP at 2 months | 89.9 (7.8) | 93.3 (8.5) | 93.2 (14.7) | 96 (12.8) | – | – | 92.7 (7.4) | 95.5 (8.1) |
| Nighttime ambulatory systolic BP at 2 months | 125.6 (12.8) | 129.4 (13.1) | 126.3 (18.4) | 76.2 (12.2) | – | – | 125.5 (15.0) | 132.4 (12.2) |
| Nighttime ambulatory diastolic BP at 2 months | 74.8 (8.5) | 77.3 (8.5) | 131.9 (20.9) | 78.4 (13.2) | – | – | 75.1 (9.7) | 79.6 (7.5) |
|
BP, blood pressure; GFR, glomerular filtration rate; SD, standard deviation; uRDN, ultrasound renal denervation. |
||||||||
Table 2. Summary of included studies
| Study ID | Country | Study design | Total population | Compare interventions | Key findings |
|---|---|---|---|---|---|
| United States/Europe | RCT | 146 | uRDN vs SHAM control | Renal denervation resulted in a greater reduction in daytime ambulatory systolic blood pressure compared with a sham procedure | |
| United States/Europe | RCT | 136 | uRDN vs SHAM control | Renal denervation reduced daytime ambulatory systolic blood pressure more than the sham procedure | |
| Japan and South Korea | RCT | 136 | uRDN vs SHAM control | Is the first trial of ultrasound renal denervation in Asian patients with hypertension on antihypertensive therapy | |
| The study did not show a significant difference in ambulatory blood pressure reductions in treated patients with resistant hypertension | |||||
| United States | RCT | 224 | uRDN vs SHAM control | The primary efficacy outcome was the mean change in daytime ambulatory SBP at 2 months | |
| No major adverse events were reported in either group | |||||
|
RCT: randomized controlled trial; SBP, systolic blood pressure; uRDN: ultrasound renal denervation. |
|||||
In the analysis of 642 patients, the mean age was 54.15 years ± 9.95, 70.8% were men, and the mean body mass index was estimated at 30 kg/m2 ± 5.3. Regarding comorbidities, 15.1% had type 2 diabetes mellitus, and 5.6%, cardiovascular disease. The mean glomerular filtration rate (GFR) was estimated at 82.25 mL/min/1.73 m2 ± 16.2. In addition, 9.6% of patients had GFR levels < 60 mL/min/1.73 m2. Of note, eligibility criteria in all trials include an estimated GFR > 40 mL/min/1.73 m2. Two studies— the RADIANCE-HTN SOLO and the RADIANCE II—included patients on 1 to 3 antihypertensive drugs and were designed as “Off Med” studies, meaning patients underwent a washout period with no antihypertensive treatment for 4 weeks in the RADIANCE-HTN SOLO and 8 weeks in the RADIANCE II. Additionally, patients who experienced complications such as high BP were given antihypertensive escape therapy.26 On the other hand, the RADIANCE-HTN TRIO and REQUIRE trials included patients on 3 to 5 antihypertensive drugs and evaluated the uRDN in patients on concomitant antihypertensive therapy. However, only the RADIANCE-HTN TRIO trial standardized antihypertensive treatment over a 4-week regimen with a fixed-dose of 3 drugs in a single pill including amlodipine 10 mg; valsartan 160 mg (or olmesartan 40 mg); and hydrochlorothiazide 25 mg. Additionally, treatment adherence was assessed by mass spectrometry.21,27,28 Enrollment criteria were comparable across the analyzed studies. Similarly, exclusion criteria were consistent in all studies; however, the RADIANCE trials additionally excluded patients with anatomical variations or alterations in renal artery anatomy, as detected on renal computed tomography or magnetic resonance angiography.27 In all studies, patients were blinded prior to the uRDN procedure. Furthermore, in all RADIANCE trials, blinding was implemented after the washout period or after the patients completed the fixed-dose treatment.18,26,27
Daytime ambulatory blood pressure
Patients treated with uRDN for up to 2 months experience a significant reduction of −5.12 mmHg (95%CI, −6.07 to −4.17; P < .00001); I2 = 2%) in daytime ambulatory SBP vs the sham group. Similarly, ambulatory diastolic blood pressure (DBP) dropped down to −2.82 mmHg (95%CI, −3.43 to −2.21; P < .00001; I2 = 0%) in patients with uRDN vs the sham group (figure 2A).

Figure 2. Meta-analysis of the effect of uRDN on blood pressure va a sham control. A: difference in daytime ambulatory BP up to 2 months; B: difference in 24-hour BP up to 2 months; C: difference in office BP up to 2 months; and D: difference in home BP up to 2 months. Forest plots showing the mean difference and SD from random assignments between the uRDN and sham control groups. 95%CI, 95% confidence interval; BP, blood pressure; SD, standard deviation; uRDN, ultrasound renal denervation. The bibliographical references mentioned in this figure correspond to Azizi et al.,16-18 and Kario et al.21
24-hour ambulatory blood pressure
24-h BP was evaluated up to 2 months after uRDN. Analysis of SBP showed a significant reduction of −4.87 mmHg (95%CI, −6.53 to −3.21; P < .00001; I2 = 42%). Meanwhile, 24-h DBP dropped down to −2.55 mmHg (95%CI, −3.83 to −1.26; P < .00001; I2 = 62%) in patients on uRDN (figure 2B).
Office blood pressure
SBP dropped down to −5.03 mmHg after 2 months (95%CI, −6.27 to −3.79; P < .00001; I2 = 0%) in uRDN patients. DBP showed a significant decrease of −3.68 mmHg (95%CI, −4.57 to −2.78; P < .00001; I2 = 31%) with the uRDN intervention (figure 2C).
Home blood pressure
Analysis of home BP after 2 months showed a decrease in SBP of −5.47 mmHg (95%CI, −8.08 to −2.85; P < .0001; I2 = 75%), while DBP dropped down to −3.19 mmHg (95%CI, −4.63 to −1.75; P < .0001; I2 = 69%) in patients on uRDN (figure 2D).
Nighttime blood pressure
Nighttime BP was evaluated at the 2-month follow-up. We found that SBP dropped down to −3.99 mmHg (95%CI, −7.00 to −0.99; P = 0.009; I2 = 70%), while DBP dropped down to −2.30 mmHg (95%CI −4.03 to −0.56; P = .01; I2 = 64%) in patients on uRDN (figure 2 of the supplementary data).
Drugs 6 months after uRDN
Patient drugs 6 months after uRDN were only reported in the RADIANCE-HTN SOLO and RADIANCE-HTN TRIO clinical trials. Data analysis revealed that uRDN leads to using fewer antihypertensive drugs by −0.52 (95%CI, −0.91 to −0.13; P = 0.009; I2 = 69%) vs the sham control group (figure 3).
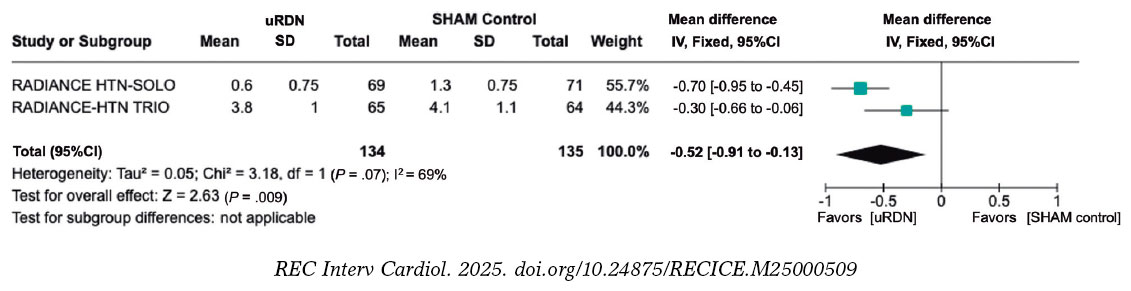
Figure 3. Patients on uRDN used less antihypertensive medication prescribed 6 months after the procedure vs the sham group. 95%CI, 95% confidence interval; BP, blood pressure; SD, standard deviation; uRDN, ultrasound renal denervation. The bibliographical references mentioned in this figure correspond to Azizi et al.16 and Azizi et al.17
Risk of bias assessment
Among the 4 studies included, the risk of bias remained consistent at a moderate level, which was attributed to the inability to blind the interventional cardiologist conducting the uRDN, although outcome assessors were blinded to the interventions performed. Studies were categorized as having moderate risk16-18,21 (table 3). Data on risk of bias can be found in table 1 of the supplementary data. In addition, the funnel plot of daytime ambulatory SBP (figure 1 of the supplementary data) showed a slight asymmetry, as points tend to concentrate towards the left side of the combined effect, which could suggest a possible publication bias. In addition, the points closer to the vertex represent studies with lower standard error due to a larger sample size. The heterogeneity of the funnel plot reflects variations in effects across studies. Plot points are within the funnel lines, but one of them towards the lower right seems further away from the rest, which could indicate a possible outlier or methodological or population differences.29
Table 3. Risk of bias summary for randomized studies (RoB 2)
| Trials | Risk of bias domains | |||||
|---|---|---|---|---|---|---|
| D1 | D2 | D3 | D4 | D5 | Overall | |
| RADIANCE HTN SOLO16 | Low | Low | Low | Low | Low | Low |
| RADIANCE HTN TRIO17 | Low | Low | Low | Low | Low | Low |
| REQUIRE21 | Low | Low | Low | Low | Low | Low |
| RADIANCE II18 | Some concerns | Low | Low | Low | Low | Some concerns |
|
D1: bias arising from the randomization process. D2: bias due to deviation from intended intervention. D3: bias due to missing outcome data. D4: bias in outcome measurement. D5: bias in selection of the reported result. |
||||||
DISCUSSION
This meta-analysis includes data from 4 randomized controlled trials that evaluated the efficacy profile of uRDN in patients with true resistant hypertension and off-medication hypertensive patients vs a sham group. Antihypertensive efficacy was evaluated across different clinical settings such as 24-h ambulatory BP, home BP, office BP, and daytime BP. Our results demonstrated significant BP-lowering efficacy at the 2-month follow-up vs the sham procedure. Furthermore, at the 6-month follow-up, fewer antihypertensive drugs were prescribed to patients on uRDN vs those from the sham group. These results support the use of uRDN as an adjuvant therapy for hypertension and as a valuable option for reducing BP as well as the number of antihypertensive drugs.
Previous studies have demonstrated the safety profile of RDN for the treatment of resistant hypertension, such as the first-generation SIMPLICITY HTN trials.30 However, the SIMPLICITY HTN-3 study showed no differences in the 24-h BP reduction vs the sham group, casting doubts on the benefits of RDN.14 Subsequently, new catheters were developed for performing RDN, and standardized criteria were established for conducting RDN trials with a sham group.12,19 Currently, uRDN has emerged as a novel option as an adjuvant therapy treatment of hypertension. It is based on catheter systems, such as the TIVUS and Paradise systems, which utilize ultrasound energy for the thermal ablation of afferent and efferent renal nerves.19,31
Our results demonstrated a reduction in both SBP and DBP at the 2-month follow-up, with a more pronounced effect on SBP in patients on uRDN vs the sham control group. We observed a reduction of −5.12 mmHg in ambulatory SBP, −4.87 mmHg in 24-h SBP, −5.03 mmHg in office SBP, and −5.47 mmHg in home SBP. These findings are particularly relevant since SBP has turned out to be a strong predictor of future cardiovascular events and mortality, regardless of age in adults.32 The CI values for home BPS had the widest range. Furthermore, the RADIANCE HTN-SOLO trial demonstrated a wide CI in both office and home SBP. This observation is an opportunity for future trials to focus on patient training to standardize home BP measurement since day-to-day home BP has been proposed as a potential predictor of cardiovascular disease.33
Although the observed BP reduction may seem minimal and lack significant clinical relevance, it is important to note that these findings reflect the first 2 months of follow-up after uRDN initiation and literature reports that uRDN has a sustained long-term effect on lowering BP values. For example, the HTN RADIANCE-SOLO trial demonstrated that at the 36-month follow-up, office BP decreased 18/11 ± 15/9 mmHg.34 Related to this, previous studies have demonstrated that a 10 mmHg reduction in SBP is associated with a decrease in the relative risk (RR) of major cardiovascular events (RR, 0.80; 95%CI, 0.77-0.83), coronary heart disease (RR, 0.83; 95%CI, 0.78-0.88), stroke (RR, 0.73; 95%CI, 0.68-0.77), heart failure (RR, 0.72; 95%CI, 0.67-0.78), and a 13% reduction in all-cause mortality rate (RR, 0.87; 95%CI 0.84-0.91).2 However, it has recently been reported that even a 5 mmHg decrease is beneficial to reduce the risk of major cardiovascular events, estimating a hazard ratio (HR) of 0.91 (95%CI, 0.89-0.94) for individuals without previous cardiovascular disease and a HR of 0.89 (95%CI, 0.86-0.92) for those with previous cardiovascular disease.1 In addition, reduction of preventable major cardiovascular events by treating hypertension has a positive economic impact in reducing hospitalization expenses due to complications such as heart attack or stroke.35 Hypertension is a prevalent global health concern, and effective BP control is achieved in only 21% of patients.36 In the United States, individuals with hypertension are estimated to incur an additional $2500 to $3000 in annual expenses vs those without hypertension. Maintaining normal BP not only benefits patients but also supports the economic well-being of the entire health care system.37 In fact, studies evaluating the cost-effectiveness of long-term use of radiofrequency RDN have been conducted in the United States and the United Kingdom concluding that this procedure represents a cost-effective option for the treatment of uncontrolled and resistant hypertension, as its sustained BP-lowering effect favors the reduction of cardiovascular morbidity and mortality.38 Similarly, in Spain, an estimate was made of the impact of radiofrequency RDN on quality-adjusted life years, cardiac events, and patient-related lifetime costs. Radiofrequency RDN was found to reduce the risk of stroke (RR, 0.80), myocardial infarction (RR, 0.88), and heart failure (RR, 0.72) throughout a 10-year period, resulting in improved health outcomes and long-term cost savings. Results presented indicate that radiofrequency RDN is a cost-effective therapeutic option that should be taken into consideration in patients with uncontrolled hypertension, including resistant hypertension.39
In addition to the reduction in BP and the positive cost-effectiveness of uRDN, radiofrequency RDN has been demonstrated to be a safe procedure for the patients. The clinical trials that analyzed this meta-analysis found no safety differences between the treated and sham groups. Furthermore, few postoperative adverse events were reported. Most complications were associated with back pain, which was effectively and uneventfully managed.16-18,21 The long-term safety profile of the procedure has been consistently reported, with no adverse effects being reported from uRDN observed at the 1, 3-, and even 8-year follow-up.34,40,41
Our findings also demonstrated that, at the 6-month follow-up, patients on uRDN used fewer prescribed antihypertensive drugs, which suggests that treatment may potentially improve patient outcomes. However, this outcome was only evaluated in the RADIANCE HTN-TRIO and RADIANCE HTN-SOLO trials. In addition, at the 3-year follow-up the RADIANCE HTN-TRIO reported no differences in the number of drugs used by patients initially identified with uncontrolled hypertension, although they decreased office SBP by 10.8 mmHg.34 This is particularly noteworthy as non-adherence to therapy is a significant contributing factor to uncontrolled BP.42 However, the results suggest that the greatest benefit is observed in the maintenance of low BP levels rather than in the decrease in the number of antihypertensive drugs prescribed.
Of note, the I2 value of the outcomes evaluated showed that daytime SBP and DBP had low heterogeneity, while the 24-h SBP and DBP values had moderate-to-high heterogeneity. On the other hand, office SBP and DBP had low-to-moderate heterogeneity. Finally, home SBP and DBP, as well as nighttime SBP and DBP and drug intake had high heterogeneity. Variations in heterogeneity do not necessarily indicate that the results are not useful;43 possibly, the differences in the heterogeneity of the outcomes assessed is due to differences in the methodology of the studies contemplated in this meta-analysis, which will be discussed below.
Our analysis included the REQUIRE trial, which has certain limitations, such as the absence of a blinded design, a non-standardized uRDN intervention, and dose titration. These factors may have introduced bias, potentially explaining the lack of differences observed between the uRDN and sham groups. In addition, the inclusion criteria of the study did not consider the presence of anatomical variations in the renal arteries vs the RADIANCE trials in which an exclusion criterion is the presence of anatomical variations in renal arteries. This factor, along with therapeutic adherence, could impact the BP reduction results.21,28,44 Based on this perspective, the European Society of Cardiology (ESC) Council on Hypertension and the European Association of Percutaneous Cardiovascular Interventions (EAPCI) have established the characteristics that must be met by studies evaluating RDN with a sham control group to be considered as high quality: a) multicenter design; b) blinding of patients; c) ambulatory BP change as the primary enpoint; d) use of second-generation RDN systems.10 In this context, RADIANCE clinical trials are characterized by a rigorous methodological protocol, which required a 4- or 8-week stabilization of pharmacological therapy prior to randomization to either uRDN or a sham procedure.45,46 Furthermore, RADIANCE trials monitored therapeutic adherence and were designed to assess the effect of uRDN with and without antihypertensive treatment, minimizing the confounding effects.28,47
A key long-term challenge of the RADIANCE trials is to demonstrate sustained BP-lowering effects vs sham groups. Follow-up studies show that patients from the sham group required higher doses of antihypertensive drugs, while those on uRDN used fewer drugs. Although BP differences across groups decreased throughout time, uRDN patients consistently needed fewer prescriptions.26,27
Results from the RADIANCE trials demonstrate the efficacy profile of uRDN for the treatment of resistant hypertension and patients with poor therapeutic adherence, as observed in the off-study population. Additionally, the REQUIRE trial highlights the potential role of anatomical variations in determining patient suitability for uRDN, underscoring the importance of selecting appropriate criteria for patient selection. In addition, RDN has proven to be a safe procedure with a positive long-term cost-benefit ratio. The key question on uRDN may be: Which patient group would benefit most from uRDN, considering anatomical factors and therapeutic adherence?
Study limitations
To make the most out of the study results, it is important to consider its limitations: a) we only analyzed data from trials that used uRDN, which reduces the size of the population; b) data availability from the studies considered covered a short follow-up period, which limits the ability to determine the long-term antihypertensive efficacy of uRDN; c) differences in supervised drug adherence across the methodological designs limit their applicability to real-world settings; d) Since RCTs included patients with true resistant hypertension and off-med hypertension, the heterogeneous population limits the generalizability of the results to a specific hypertension subtype; and e) The funnel plot showed asymmetry, suggesting a possible publication bias, although results should be interpreted with caution because the funnel plot also indicates that there is a limited amount of data.
CONCLUSIONS
This meta-analysis demonstrates that uRDN treatment effectively reduces both SBP and DBP across various contexts, including 24-h, ambulatory, home and office BP at the initial 2-month follow-up in hypertensive patients (figure 4). Additionally, uRDN was associated with reduced antihypertensive drug use 6 months after the procedure. However, further research is needed to assess its long-term effects and identify the patient groups who may benefit the most.

Figure 4. Central illustration. Summary of the effect on the decrease in systolic and diastolic blood pressure in patients on uRDN compared with patients who received the sham procedure at the 2 months postoperative follow-up. uRDN, ultrasound renal denervation.
FUNDING
This manuscript did not receive financial support from any institution or funding agency for its preparation.
ETHICAL CONSIDERATIONS
The present meta-analysis was conducted based on previously published studies. As the study involved secondary data analysis, no new data was collected from human participants or animals, and the use of SAGER guidelines does not apply to this study. Therefore, ethical approval was deemed unnecessary. All included studies were reviewed in full compliance with ethical guidelines set forth by the respective institutions where the original studies were conducted. All authors state that the data used in this study were obtained exclusively from publicly accessible sources, and no confidential or proprietary information was utilized without appropriate authorization.
STATEMENT ON THE USE OF ARTIFICIAL INTELLIGENCE
During the preparation of this work the authors used ChatGPT-4o to review the document syntaxis and grammar. After using this tool/service, the authors reviewed and edited the content as needed and took full responsibility for the content of the published article.
AUTHORS’ CONTRIBUTIONS
J.M. Guerrero-Hernández: conceptualization, formal analysis, drafting, review and editing; C. J. Palomino-Ojeda: methodology, investigation, drafting, review and editing; L. H. García-Mena: methodology, formal analysis, writing, review and editing; Ó.Á. Vedia-Cruz: investigation; J. L. Maldonado-García: drafting, review and editing; I. J. Núñez-Gil: investigation, supervision and review; J. A. García-Donaire: review and supervision.
CONFLICTS OF INTEREST
I. J. Núñez-Gil served as a consultant for Medtronic and Recor Medical in the denervation field. J. A. García-Donaire served as consultant for Medtronic and Recor Medical in the denervation field. The rest of the authors declared no conflicts of interest whatsoever.
WHAT IS KNOWN ABOUT THE TOPIC?
- uRDN has emerged as a safe option for the treatment of resistant hypertension, and previous studies have observed greater efficacy in lowering BP vs a sham group.
WHAT DOES THIS STUDY ADD?
- Our results demonstrate that uRDN decreased 24-h, office, daytime and home SBP and DBP within the first 2 months after the procedural follow-up vs a sham group, and a decrease in the number of antihypertensive drugs at the 6-month follow-up. However, further long-term studies are required to confirm the benefit of uRDN.
SUPPLEMENTARY DATA

REFERENCES
1. Adler A, Agodoa L, Algra A, et al. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure:an individual participant-level data meta-analysis. The Lancet. 2021;39:1625-1636.
2. Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death:A systematic review and meta-analysis. The Lancet. 2016;387:957-967.
3. Carey RM, Muntner P, Bosworth HB, Whelton PK. Prevention and Control of Hypertension:JACC Health Promotion Series. J Am Coll Cardiol. 2018;72:1278-1293.
4. Choudhry NK, Kronish IM, Vongpatanasin W, et al. Medication adherence and blood pressure control:A scientific statement from the american heart association. Hypertension. 2022;79:E1-E14.
5. Egan BM, Zhao Y, Li J, et al. Prevalence of optimal treatment regimens in patients with apparent treatment-resistant hypertension based on office blood pressure in a community-based practice network. Hypertension. 2013;62:691-697.
6. Flack JM, Buhnerkempe MG, Moore KT. Resistant Hypertension:Disease Burden and Emerging Treatment Options. Curr Hypertens Rep. 2024;26:183-199.
7. Grassi G, Ram VS. Evidence for a critical role of the sympathetic nervous system in hypertension. J Am Soc Hypertens. 2016;10:457-466.
8. Mabin T, Sapoval M, Cabane V, Stemmett J, Iyer M. First experience with endovascular ultrasound renal denervation for the treatment of resistant hypertension. EuroIntervention. 2012;8:57-61.
9. Dasgupta I, Sharp ASP. Renal sympathetic denervation for treatment of hypertension:where are we now in 2019? Curr Opin Nephrol Hypertens. 2019;28:498-506.
10. Barbato E, Azizi M, Schmieder RE, et al. Renal denervation in the management of hypertension in adults. A clinical consensus statement of the ESC Council on Hypertension and the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2023;44:1313-1330.
11. Rodríguez-Leor O, Jaén-Águila F, Segura J, et al. Renal denervation for the management of hypertension. Joint position statement from the SEH-LELHA and the ACI-SEC. REC Interv Cardiol. 2022;4:39-46.
12. Schmieder R, Burnier M, East C, Tsioufis K, Delaney S. Renal Denervation:A Practical Guide for Health Professionals Managing Hypertension. Interv Cardiol. 2023;18:e06.
13. Azizi M, Sapoval M, Gosse P, et al. Optimum and stepped care standardised antihypertensive treatment with or without renal denervation for resistant hypertension (DENERHTN):a multicentre, open-label, randomised controlled trial. Lancet. 2015;385:1957-1965.
14. Bhatt DL, Kandzari DE, O'Neill WW, et al. A Controlled Trial of Renal Denervation for Resistant Hypertension. N Engl J Med. 2014;370:1393-1401.
15. Stiermaier T, Okon T, Fengler K, et al. Endovascular ultrasound for renal sympathetic denervation in patients with therapy-resistant hypertension not responding to radiofrequency renal sympathetic denervation. EuroIntervention. 2016;12:e282-e289.
16. Azizi M, Schmieder RE, Mahfoud F, et al. Endovascular ultrasound renal denervation to treat hypertension (RADIANCE-HTN SOLO):a multicentre, international, single-blind, randomised, sham-controlled trial. Lancet. 2018;391:2335-2345.
17. Azizi M, Sanghvi K, Saxena M, et al. Ultrasound renal denervation for hypertension resistant to a triple medication pill (RADIANCE-HTN TRIO):a randomised, multicentre, single-blind, sham-controlled trial. Lancet. 2021;397:2476-2486.
18. Azizi M, Saxena M, Wang Y, et al. Endovascular Ultrasound Renal Denervation to Treat Hypertension:The RADIANCE II Randomized Clinical Trial. JAMA. 2023;329(8):651-661.
19. Lauder L, Kandzari DE, Lüscher TF, Mahfoud F. Renal denervation in the management of hypertension. EuroIntervention. 2024;20:E467-E478.
20. Reuter E. The FDA approved 2 renal denervation devices. There are still questions about who will benefit. MedTech Dive. 13 Dec 2023. Available at:https://www.medtechdive.com/news/renal-denervation-recor-medtronic-evidence/702385/. Accessed 20 Dec 2024.
21. Kario K, Yokoi Y, Okamura K, et al. Catheter-based ultrasound renal denervation in patients with resistant hypertension:the randomized, controlled REQUIRE trial. Hypertens Res. 2022;45:221-231.
22. Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Cochrane;2023. Avalilable at:https://training.cochrane.org/handbook. Accessed 1 Dec 2024.
23. Sterne JAC, Savovic´J, Page MJ, et al. RoB 2:a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366.
24. Wilson DB. Practical meta-analysis effect size calculator (Version 2023.11.27). 2023. Available at:https://www.campbellcollaboration.org/calculator/d-ordinal-freq. Accessed 20 Dec 2024.
25. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177-188.
26. Azizi M, Schmieder RE, Mahfoud F, et al. Six-Month Results of Treatment-Blinded Medication Titration for Hypertension Control After Randomization to Endovascular Ultrasound Renal Denervation or a Sham Procedure in the RADIANCE-HTN SOLO Trial. Circulation. 2019;139:2542-2553.
27. Azizi M, Mahfoud F, Weber MA, et al. Effects of Renal Denervation vs Sham in Resistant Hypertension After Medication Escalation:Prespecified Analysis at 6 Months of the RADIANCE-HTN TRIO Randomized Clinical Trial. JAMA Cardiol. 2022;7:1244.
28. Mauri L, Kario K, Basile J, et al. A multinational clinical approach to assessing the effectiveness of catheter-based ultrasound renal denervation:The RADIANCE-HTN and REQUIRE clinical study designs. Am Heart J. 2018;195:115-129.
29. Sterne JAC, Sutton AJ, Ioannidis JPA, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. 2011;343:d4002.
30. Epstein M, De Marchena E. Is the failure of SYMPLICITY HTN-3 trial to meet its efficacy endpoint the “end of the road“for renal denervation? J Am Soc Hypertens. 2015;9:140-149.
31. Haribabu S, Sharif F, Zafar H. Recent trends in renal denervation devices for resistant hypertension treatment. Ir J Med Sci. 2021;190:971-979.
32. McCarthy CP, Natarajan P. Systolic Blood Pressure and Cardiovascular Risk:Straightening the Evidence. Hypertension. 2023;80:577-579.
33. Kario K, Kanegae H, Okawara Y, Tomitani N, Hoshide S. Home Blood Pressure Variability Risk Prediction Score for Cardiovascular Disease Using Data From the J-HOP Study. Hypertension. 2024;81:2173-2180.
34. Rader F, Kirtane AJ, Wang Y, et al. Durability of blood pressure reduction after ultrasound renal denervation:three-year follow-up of the treatment arm of the randomised RADIANCE-HTN SOLO trial. EuroIntervention. 2022;18:E677-E685.
35. Wang G, Grosse SD, Schooley MW. Conducting Research on the Economics of Hypertension to Improve Cardiovascular Health. Am J Prev Med. 2017;53(6 Suppl 2):S115.
36. Kario K, Okura A, Hoshide S, Mogi M. The WHO Global report 2023 on hypertension warning the emerging hypertension burden in globe and its treatment strategy. Hypertens Res. 2024 47:5. 2024;47:1099-1102.
37. Kumar A, He S, Pollack LM, et al. Hypertension-Associated Expenditures Among Privately Insured US Adults in 2021. Hypertension. 2024;81:2318-2328.
38. Taylor RS, Bentley A, Metcalfe K, et al. Cost Effectiveness of Endovascular Ultrasound Renal Denervation in Patients with Resistant Hypertension. Pharmacoecon Open. 2024;8:525.
39. Rodríguez-Leor O, M. Ryschon A, N. Cao K, et al. Cost-effectiveness analysis of radiofrequency renal denervation for uncontrolled hypertension in Spain. REC Interv Cardiol. 2024;6:305-312.
40. M Zeijen VJ, Völz S, Zeller T, et al. Long-term safety and efficacy of endovascular ultrasound renal denervation in resistant hypertension:8-year results from the ACHIEVE study. Clin Res Cardiol. 2024. https://doi.org/10.1007/s00392-024-02555-7.
41. Azizi M, Daemen J, Lobo MD, et al. 12-Month Results From the Unblinded Phase of the RADIANCE-HTN SOLO Trial of Ultrasound Renal Denervation. JACC Cardiovasc Interv. 2020;13:2922-2933.
42. Hamrahian SM, Maarouf OH, Fülöp T. A Critical Review of Medication Adherence in Hypertension:Barriers and Facilitators Clinicians Should Consider. Patient Prefer Adherence. 2022;16:2749.
43. Borenstein M. How to understand and report heterogeneity in a meta-analysis:The difference between I-squared and prediction intervals. Integr Med Res. 2023;12:101014.
44. Kario K, Kai H, Nanto S, Yokoi H. Anti-hypertensive medication adherence in the REQUIRE trial:post-hoc exploratory evaluation. Hypertens Res. 2023;46:2044-2047.
45. Mahfoud F, Azizi M, Ewen S, et al. Proceedings from the 3rd European Clinical Consensus Conference for clinical trials in device-based hypertension therapies. Eur Heart J. 2020;41:1588-1599.
46. Kandzari DE, Mahfoud F, Weber MA, et al. Clinical Trial Design Principles and Outcomes Definitions for Device-Based Therapies for Hypertension:A Consensus Document From the Hypertension Academic Research Consortium. Circulation. 2022;145:847-863.
47. Kandzari DE, Mahfoud F, Bhatt DL, et al. Confounding Factors in Renal Denervation Trials:Revisiting Old and Identifying New Challenges in Trial Design of Device Therapies for Hypertension. Hypertension. 2020;76:1410-1417.












